English I – Unit 10 Review Library Skills and Visual Aids
Sickle cell disorders (SCD) are a grouping of chronic inherited claret atmospheric condition. The majority of studies on SCD have a clinical focus and bargain with how those living with SCD 'manage' what is constructed as a given: the 'status' of SCD. Consequently, many studies present the psychological touch on, referring uncritically to what are termed 'coping strategies'. Current debates on SCD and other chronic conditions rarely engage with the broader social context. In part response to this, our paper presents a critical review of the literature on SCD, young people and education. The newspaper evaluates literature that touches on education and SCD, before last with a broad discussion of future research and policy priorities. Throughout, we reflect on how the process of constructing a cognition base of operations from available literature is problematic. Nosotros specifically discuss how electric current research presents a skewed pic of the experience of SCD, which is of limited value to those responsible for instruction policy and do. The paper concludes that research should move beyond describing the basic health needs of people with SCD by including the social context of their lives. Existing literature on the individual educational experiences of immature people living with SCD is, however, either dated or limited past being based on conceptual argument rather than empirical data. Consequently, there is a need for well-designed studies to establish the best way to come across the educational needs of young people with SCD, reflecting not only their wellness needs in schoolhouse, but the whole context of living with SCD, including interaction with disabling or racist structures. Furthermore, this holistic approach could contribute to a wider understanding of the educational needs of immature people from minority ethnic backgrounds and of young people living with chronic illnesses.
Fundamental words
chronic illness, education, England, sickle cell, social context, young people
Introduction
Sickle cell disorders (SCD) are chronic inherited blood atmospheric condition affecting people from all indigenous groups, but particularly those of African, African-Caribbean, Mediterranean, Center Eastern and Indian descent (Serjeant, 2001). Altogether, 21.4% of the primary school population in England record their ethnic origin in groups at higher take chances of sickle jail cell (Department for Education and Skills, 2006). Thus, even without further inward migration or differential fertility, the future school population of England will comprise over one-fifth of pupils at higher risk of carrying genes associated with SCD, which is maybe non surprising given that SCD is the most common genetic condition in the Great britain.
This newspaper presents a knowledge review on education and young people with SCD. There is comparatively little written straight on education. Rather, most SCD literature that either touches on education and/or has implications for teaching adopts a medical model, with education subordinated to the clinical consequences of the condition (see Anionwu and Atkin, 2001). We wish to transcend clinical approaches to chronic illness and focus more on the socio-cultural context of immature people with SCD.

Table 1 :Databases searched and search strategy
A noesis review differs fundamentally from a systematic review. The latter is less suited to exploring the broader context in which testify is produced, especially when faced with a contested area, such as ethnicity and SCD, where the focus of the actual inquiry is often questioned, or is scarce, or is subordinated to other concerns (encounter Atkin and Chattoo, 2007). Moreover, we are concerned non simply to present what the literature tells us, but too to interrogate it critically, so that the assumptions in the production of literature themselves become part of the analytical process (see Popay and Roen, 2003; Sellick and Howell, 2003).
Conducting the knowledge review
Nosotros adopted a systematic arroyo to collecting the material (see Samanta et al, 2005), although in analysing and writing upwards our findings, our approach was informed by knowledge review procedures adult by the Social Care Establish for Excellence (2007).Knowledge reviews provide a thematic exploration of the relevant literature, which can be useful in informing policy, especially when the evidence base for information is weak (Atkin et al, 2006).
The principal review questions were:
• What experiences in education do young people with SCD have?
• How do education services respond to the needs of pupils with SCD and their carers?
• What makes appropriate educational support for young people with SCD and their carers?
• To what extent exercise young people's specific experiences of education relate to the broader experience of SCD?
The inclusion criteria for the review were that the cloth met at least one of the guiding review questions, waswritten in English language, andwas published betwixt 1972 and 2007. The exclusion criteria included literature that focused just on sickle cell carriers or exclusively on clinical management, or was in the form of dissertations, abstracts, comments, letters, editorials or book reviews. A search of literature was conducted using databases and keywords equally presented in Tabular array 1.
This search produced numerous manufactures, including, for case, ones on the education of children with SCD about clinical aspects of their condition (Katz et al, 2002) or on increasing teacher knowledge of SCD (Rex et al, 2005), only few with a specific focus on schoolhouse education and young people with SCD (come across Table 2).
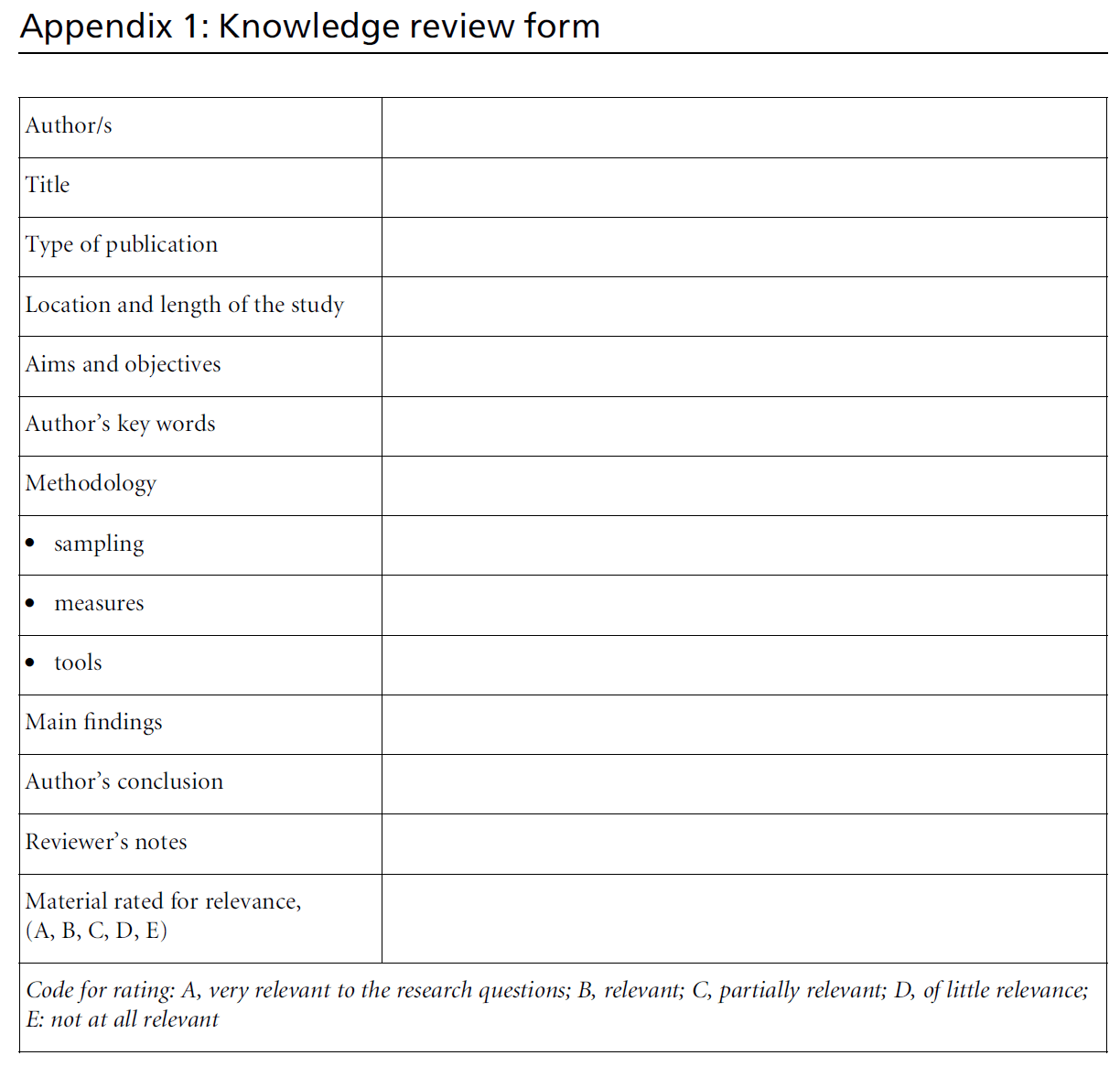
In social club to assist the retrieval of key points from the references thus identified, a standard formwas devised (see Appendix one).
A total of 332 references judged potentially relevant were entered into the EndNote database programme, and in 238 cases the abstract and keywords were besides incorporated into the database. A total of 94 full articles that met the chief search criteria of education and young people with sickle cell disorder were reviewed.
Presenting the themes identified in the literature
Nearly studies adopted psychological and clinical perspectives. The literature also positions young people with SCD inside disabling discourses, referring to their 'psychological aligning' (Hurtig and Park, 1989; Midence et al, 1993) and 'coping strategies' (Barbarin et al, 1999; Robinson, 1999; Royal et al, 2000; Thomas et al, 2001; Anie et al, 2002), with piffling recognition of the insights of the social model of inability (Oliver, 1990). This highlights how taking existing literature as 'what we know' presents a skewed picture of the feel of those with SCD, because information technology does not explore the social context in which the condition (or indeed the production of knowledge) occurs.
An appraisement of existing accounts
Discrimination arising from SCD, equally with whatsoever other chronic illness, has an impact on immature people'due south social life. Nevertheless, the implications of this vary between individuals, different age groups, gender, and the socio-economic and cultural backgrounds of the young people (Darr et al, 2005). The literature, however, rarely reflects this and is dominated by psychological accounts, focusing on aligning to the condition. Farther, with the exception of Koontz et al (2004), studies involving intervention in the school surround to meliorate educational experiences were conspicuously lacking.
Isolation (Pinckney and Stuart, 2004), dependency, fear of disease, stigmatisation and hospitalisation, withdrawal from family and peers (Morgan and Jackson, 1986), poor self-image (Noll et al, 1992), depression (Barbarin et al, 1999; Rodrigue et al, 1996 ) and preoccupation with death (Boni et al, 2001) are reported equally part of the experience of what it means to be a young person with SCD. Consequently, commonly claimed psychological outcomes among young people with SCD include feelings of helplessness and worthlessness, stress, frustration, anxiety, self-blame, low self-image and esteem, low and neurocognitive impairment. Furthermore, many studies, in keeping with their initial focus, maintain the importance of utilisation of psychological intervention, and recommend farther research on patient education (Collins et al, 1998; Hasan et al, 2003; Helps et al, 2003; Barakat et al, 2006), cerebral-behavioural therapy (Anie, 2005), or special educational support to assist improve the quality of life of patients (Morgan and Jackson, 1986; Adedoyin, 1992; Midence et al, 1993, 1996; Hilton et al, 1997; Thomas et al, 2001; Thomas and Taylor, 2002; Alao and Dewan, 2003; Anie and Green, 2006). Such interventions, all the same, seem to work for some people and not others, being sensitive to the context in which they are introduced (see Atkin et al, 2006).

Table 2:Search outcomes for databases: number of articles constitute.
What is credible from the review is the absenteeism of whatsoever lucent association betwixt disease severity and outcomes (Barbarin et al, 1994; Burlew et al, 2000). Some individualswith SCDmight develop psychological problems, but others do non (Burlew et al, 2000), consistent with the full general literature on chronic affliction (see Wjst et al, 1996; Bury et al, 2005). Social factors account for more than variability than the severity of the disease per se (Burlew et al, 2000). To be of value in agreement the experience of education this needs further investigation, and we return to this when nosotros talk over the social context.
Some studies treat gender every bit a variable determining experience. For instance, girls demonstratemore 'adaptive' behaviour than boys, who testify somatic, young, and cognitive deficits to a greater caste than their female person counterparts (Brown et al, 1993). Information technology is also argued that girls are better at withstanding the challenges of SCD (Anie and Green, 2006). However, Hill (1994) provides a sociological explanation for this. She proposes that mothers did not perceive SCD as a claiming or limitation for their daughters, who were 'imagined' every bit more able and more likely to intendance for themselves than boys. Further, the social expectations of both boys and girls are different, with boys expected to exist ambitious, strong, masculine, and physically active, peculiarly in sport. In the case of young people with SCD the effects of being black, poor and/or perceived equally physically weak increase the significance of these norms and eliminate viable alternatives. The protectiveness of mothers towards sons, for example, suggests culturally synthetic gender norms that view black males equally less capable of self-intendance, independent andmore vulnerable to danger and risks. The gender care-giving strategies of some mothers, and the adverse touch of SCD on the lives of boys, reverberate the narrow range of acceptable gender office options available to low-income black male person children (Hill and Zimmerman, 1995).
This reflects broader findings that socialisation and gender expectations differ between boys and girls, and may bear on their evolution and how they perceive their illness (see Williams, 2000).Wenow consider the wider implications of this when interpreting the literature. As we have seen, much of the work in this surface area does not locate the experiences of young people with SCD inside a broader social context, including the contexts of disability bigotry, racism, and socioeconomic condition, and volition tend to list such negative characteristics equally inevitable by-products of living with SCD, rather than as constituted through social structures that are particular to time and place.
At that place are many studies that claim SCD has a significant bear on on social functioning including emotional (Noll et al, 1996), recreational and educational (Robinson, 1999; Thomas et al, 2001; Peterson et al, 2005), and vocational activities (Palermo et al, 2004). The problem with such studies, however, is that they assert either a form of biological reductionism (the life of someone with SCD reduced to their 'condition'), or a type of psychological reductionism, in which the role of discriminatory structures, racism, poverty, and the lack of legislative and policy frameworks in supporting the lives of young people with SCD are ignored. Many of these studies lack comparators with either other young people, those living with chronic affliction, or others experiencing racism. Immature people with SCD face the same challenges faced by all young people, and although having a chronic illness can brand the negotiation of being a immature person more than difficult, it does not necessarily dominate a person's identity (Atkin and Ahmad, 2001).
Towards a sociological account
There appears to be lilliputian recognition in many accounts of the extent to which the declared psychological concomitants of SCD disappear when social interventions are fabricated. Thus, teacher and peer education on sickle cell, challenges to negative labelling, establishing measures to assist preclude crises, cognition of early signs and symptoms, and reassurance of parents past consistent activity that teachers and peers are knowledgeable and supportive are, collectively, reported to accept improved school experiences for people living with SCD (Koontz et al, 2004).
The quality of life for young people with SCD tin can be more affected by the way people around them respond to them than by their condition. Yet, without the wider consideration of disabling structures and enabling social environments, whatsoever approach seeking to positively influence the lives of adolescents with SCD ends upward promoting social adjustment (Pinckney and Stuart, 2004) with SCD reified as the cause of bug. This leaves the prevailing social structures of racism, of disability bigotry (encounter Dooley and Perkins, 1998), and of diff life chances in teaching, housing and employment, also equally the context of being a young person out of business relationship. Information technology also leaves open up the door for those young people with SCD who practise not adjust to be blamed for their circumstances.
The medical and psychological dominance of much SCD literature ways that the term 'social' itself tends to be reduced to a narrow concept of interpersonal relationships (see Rodrigue et al, 1996). Conclusions that SCD can exist disruptive to family life are disembedded from context. The black family has itself been moulded past a long history of racism, and of discrimination in employment and criminal justice (Hill, 1994). This results in high levels of alone motherhood and high levels of female participation in paid labour. Conversely, wider employment bigotry means low levels of participation in formal labour markets for blackness males, with consequences for gender relations in such communities. Overlying family forms structured by racism, there are also longstanding bug of discriminatory attitudes in health services, and confusion betwixt SCD and sickle cell carriers (see Anionwu and Atkin, 2001).
In contrast to some psychological studies, Hill (1994) and Anionwu and Atkin (2001) argue that social factors shape the course and severity of the illness. Such factors include proper admission to healthcare facilities, positive attitudes of healthcare providers, gender roles, and the employment status of the individuals. This is peradventure not surprising, equally the broader sociological literature reminds usa that social standing in a serial of hierarchies, equally well equally social support, is itself a fundamental determinant of health (Wilkinson, 1996).
The meanings of SCD and its relevance to education
What are the specific implications of these rather general debates for education? In the first instance, there are several ways in which the clinical and psychological focus of the literature finds expression in pedagogy strategies. The physical features of people with SCD are said to include small body structure, sensitivity to environmental changes such equally heat and cold, body weakness and yellowish optics (Robinson, 1999; Wilson et al, 2003). Such concerns can dominate debates nearly educational activity and schooling. When policy and practice guidance does exist, information technology tends to advise teachers about the possible physical bear upon of the status on the child's schooling (see Atkin and Ahmad, 2000). Teachers, for instance, are brash to make sure a child is not exposed to the cold afterwards going swimming, takes a rest when tired, is excused concrete exertion, or is immune to visit the toilet more than regularly than other children, because of their demand to drink plenty of fluids (see Dooley and Perkins, 1998). Such advice, although potentially helpful, tin present a one-dimensional concern with SCD, which emphasises possible physical limitation and thereby fails to recognise how people may exist embodied in different ways, inside different systems of meanings, and positioned with varying degrees of social leverage (Turner, 1996). In effect, the concrete body of the young person with SCD is essentialised in a parallel mode to the reification of their psychological experiences discussed above.
In this way, the way in which young people with SCD 'physically conform' to their illness and cope with information technology is held to exist important, peculiarly within the context of their engagement with education (Morgan and Jackson, 1986; Lee et al, 1997). However, the means in which young people with SCD perceive their concrete appearance do non depend primarily upon the severity of illness, or only on the historic period and gender of the individuals. They also depend upon the forcefulness of their social support, their socio-economic and cultural background, social constructions of the allegedly normal and imagined body, and constructions of variation from the normality as impairment (Shakespeare, 1995). By contrast, many young people and their siblings learn to live positively with SCD and normalise their lives (Purple et al, 1995; Atkin et al, 1998b). Conceptualising the experience of children inside a more than social model of disability frames people as active agents who engage with their SCD, and non as passive tragic victims of the condition (Fellow et al, 2004). We return to this in our discussion. For all the positive contributions of the social model of disability in helping to contextualise research on SCD, this approach has limitations when considering pain, for not all pain can be dissolved through enabling school environments (Hughes and Paterson, 1997). Severe pain is one of the features of SCD, and negotiating a life with both chronic and intermittent acute hurting is a claiming facing many young peoplewith SCD, including during their time at schoolhouse (Maikler et al, 2001; Palermo et al, 2004; Jacob et al, 2006). Responding to the disruption of other activities such every bit slumber, eating and socialising may likewise crave addressing within schoolhouse policies on SCD, although to be consistent with our previous arguments, such policies need to recognise the social consequences of pain, which requires management in a non-clinical environment, rather than reduce it to a clinical event.
More broadly, regular school participation is seen equally essential to children's didactics and social evolution as well as their psychosocial wellbeing (Fowler et al, 1986; Nash, 1989; Midence and Elander, 1994; Fuggle et al, 1996), only there is petty substantial research that explores these issues in particular. Interruption to schooling and peer relationships is a particular difficulty facing children with a chronic disease (Mador and Smith, 1989; Davis and Wasserman, 1992; Shapiro et al, 1995; Wjst et al, 1996; Darr et al, 2005), and indeed the onset of painful crises or other clinical complications tin disrupt didactics for those with SCD (Noll et al, 1996; Schatz et al, 2001; Koontz et al, 2004). Children with SCD may accept restrictions placed on their physical activities and usually experience fatigue that tin make it difficult physically to keep up with peers (Noll et al, 1996). School activities can be farther express by hospitalisation, clinic visits or restrictions imposed past the expectations of others (Nettles, 1994).
In interrogating the literature in item, like problems regarding focus emerge. Much literature is concerned with the poor bookish functioning and achievement of pupils with SCD, rather than commonage educational systems of support or policies (Atkin and Ahmad, 1998; Thomas and Taylor, 2002). Further, the literature on academic performance has been inconsistent and controversial. Some studies suggest that poor pedagogy outcome is a upshot of how the illness affects cognitive processes. Such studies tend to skew our understanding of the condition, specially when findings are discussed in relation to IQ – a hotly debated topic, when raised in relation to ethnic minority populations (Demaine, 1989). Other authors (Hurtig and Park, 1989; Midence et al, 1996; Richard and Burlew, 1997), nevertheless, have plant no evidence to back up a relationship between illness severity and academic achievements. These findings tend to emerge from better designed studies, which include comparator groups, as well equally having sufficient ability (encounter Atkin et al, 2006). A feature of the literature, more than more often than not, is that studies on educational attainment vary in the blazon of comparison groups used, such as clinic users, children with chronic illnesses, peer groups and siblings. Studies also offer little in the way of comparison groups or control for variables such as age, gender, ethnicity and economical condition (Barbarin et al, 1999). It is, therefore, difficult to draw whatsoever firm conclusions from such evidence.
Nonetheless, the literature raises the possibility that affected children could lose out academically and become isolated from friends and peers (Conyard et al, 1980; Armstrong et al, 1996; Maikler et al, 2001; Schatz, 2004), although response to the clinical consequences of the condition, as we accept seen, varied between individuals and, according to different authors, depends on individuals' gender, historic period, stage of disease and social and cultural background (Gil et al, 1996; Murray and May, 1998; Barry and Elander, 2002; Anie and Steptoe, 2003; Dunlop and Bennett, 2006; Swain et al, 2006). Farther, we need to avoid generalisations or the use of stereotypes in predicting how a particular person from a item culturewill express feelings of pain (Helman, 2007). Indeed, the realm of the cultural background of individuals with SCD is fraught with the danger of stereotyping, including stereotypes of allegedly different pain thresholds and of drug-seeking behaviour (Anionwu and Atkin, 2001). At that place is some bear witness that teachers might not have a person's symptoms seriously, as they think they are attention seeking or being disruptive (Atkin and Ahmad, 2000).
The school context, therefore, can be important in how a person makes sense of their illness. During schooling hours, immature people with SCD interact with their peer groups and teachers, and are influenced by how other people interact with them (Koontz et al, 2004). Immature people's positive attitude and attitudes of teachers and peers in treatment pain, for instance, makes the SCD status easier (Gil et al, 2000). More broadly, this would suggest a shift in the current focus of literature, abroad from the individual to the organisational context, which interprets and responds to a person'due south condition. In that location is fiddling literature that attempts this, and even this work is not enquiry based (Dyson, 1992).
Nonetheless, themes do emerge, and these could assistance inform futurity research as well every bit policy and practice. Bear witness suggests, for instance, that a lack of understanding on the office of schools creates many difficulties for young people and, as a issue, they ofttimes do not fulfil their potential (Chua-Lim et al, 1993; Barbarin et al, 1994; Shapiro et al, 1995; Fuggle et al, 1996; Atkin and Ahmad, 2000, 2001; Darr et al, 2005). Not exceptionally, teachers are unable to deal with potential crises at school (Midence and Elander, 1994; Broome et al, 2001). Parents annotate on the ignorance of many teachers, who feel that children exaggerate the consequences of the illness (Atkin et al, 1998a). More generally, families and individuals describe education services as unresponsive to their needs (Midence and Elander, 1994). Well-nigh young people experience their illness has affected their academic progress (Atkin and Ahmad, 2001), although they actively attempt to overcome the disruption it has caused (Fuggle et al, 1996). Neither do schools seem to offer much support in overcoming these disruptions (Midence et al, 1992; Shapiro et al, 1995; Atkin and Ahmad, 2000, 2001; Darr et al, 2005). Few schools, for example, seem to accept policies on how to reply when a kid misses schoolhouse with SCD (Darr et al, 2005), and are rarely able to offer flexible tutoring or individualised educational plans (Dooley and Perkins, 1998). Anionwu (1992) suggests greater liaison between the school, domicile and hospital particularly when the child is off sick.Holman (1997) concurs and presents a protocol that has been developed for the school nurse to assist the child in the school environment. School support programmes tin likewise help amend communicationamong family, school and healthcare providers, and some studies propose that meetings between different parties are beneficial. Individually tailored SCD school intervention programmes could accost relevant issues such as absenteeism, academic difficulties, general disease management and pain (Gil et al, 2000).
Few young people had received helpful careers advice at school (Atkin and Ahmad, 2001), despite information technology being especially important for those with a chronic affliction (Nettles, 1994), although the indifference of careers officers was sometimes attributed to racism (Brahamet al, 1992; Atkin and Ahmad, 2001). This, in turn, raises the issue of employment and employment training. People with SCD may find themselves excluded from labour markets because of a lack of support, or as a consequence of employers' ignorance, inflexibility and inability to accommodate difference (Franklin and Atkin, 1986; Barrett et al, 1988; Evans, 1998; Anionwu and Atkin, 2001; Darr et al, 2005). The potential for education to become a resource to fight such bigotry could exist the field of study of research to empathise the relationship between chronic illness, ethnicity and exclusion from labour markets (see Ali et al, 2006). Without such inquiry, it is difficult to formulate successful educational activity policies.
Discussion
There is a dearth of literature exploring the educational experience of those with SCD. The literature that does be often discusses teaching in passing, subordinated to a more than clinical or psychological focus, and is concerned with private adaptation. Such research tends to essentialise a person's experience of the illness, in which they are seen to 'manage' what is constructed every bit a given – the condition. Problems, therefore, tend to become located within the individuals rather than the context they live within.
Relying solely on such an arroyo may present a skewed account of SCD and educational activity, meaning that emerging insights demand to exist heavily contextualised, in a way that recognises that illness behaviour is role of a socially defined status. To this extent, interpretation of the show becomes as important as the evidence itself (see MacDonald, 2003) and this offers a reminder of how doing inquiry is not a neutral or objective process, but embodies contested ideas, created and given meaning through the exercise of social power at specific sites of praxis (Alvesson and Sko¨ldberg, 2000).
The limitations of the current literature propose the importance of broadening the narrow focus of current debates. This requires greater appointment with the social context within which people live their lives. Chronic conditions, such as SCD, have consequences that transcend the initial illness narrative (Nettleton, 2005). Illness is simply one attribute of a person'southward identity (Bury et al, 2005), and studies often fail to contextualise the experience of people with a chronic disease with the experience of 'being' more than by and large. For example, many immature people with SCD and their siblings learn to live positively with chronic illness and normalise their lives (Atkin et al, 1998b; Royal et al, 1995).
This begins to introduce the value of conceptualising the experience of children within a more than social model of disability, which emphasises the value of conceptualising people every bit active agents who appoint with the condition, and non as passive tragic victims of atmospheric condition such as SCD (Swain et al, 2004). Disability thus becomes a social consequence, in which systematic discrimination non only leads to relative dependence and loss of option for disabled pupils, but also excludes them from activities and roles taken for granted past the bulk of the school population (Corker and French, 1998).
The social model of disability, all the same, does have drawbacks. First, authors on disability rights and on ethnicity do not always share common ground (see Ahmad, 2000), and in this respect 'independence' may be a detail cultural construct, embodying western assumptions (Atkin and Chattoo, 2007). In education inquiry this could straight our attending to investigate, for example, the extent to which young people with SCD value being able to depend upon peers to speak up for them rather than always themselves having to repeatedly account for their SCD. 2d, the social model of inability cannot e'er explicate the lived experiences of pain, even though social responses to pain from health and social care agencies do exacerbate the consequences of the affliction and make the experience of hurting far worse for those with SCD and their families (run across Anionwu and Atkin, 2001). Research in school settings could thus be directed to finding what contexts make teachers more or less likely to believe a young child with SCD when they say they are in pain.
Pupils with SCD are subject to marginalisation, in terms of both inability structures and racism. While the health-related complications of SCD are undoubtedly challenging, enabling social environments, for case, pride in ethnic identity (Bediako, 2007), can be constructed that significantly change the affliction feel. This is all the more of import as young people spend a significant amount of their time in education settings. It is a lack of educational policies and proactive intervention on the part of teachers, rather than sickle cell per se, that may atomic number 82 to bookish failure, limited career options and negative self-images. School interventions to ameliorate student experience in schools have received limited coverage. Furthermore, there is lack of noesis and appropriate resource allocations to integrate young people with SCD in mainstream educational institutions, and questions as to whether health professionals tin bridge the gap betwixt healthcare providers, students, teachers and parents (Day and Chismark, 2006).
To found the nature and extent of disabling structures, discriminatory attitudes and racist bigotry facing young people with SCD in their education, a research programme on SCD and education is required. Evidence derived from the experiences of young people with SCD and their carers is a necessary, though non a sufficient, prerequisite to creating enabling school environments. In this respect, in that location is a further feature of the literature that hinders development of an evidence base of operations in educational activity and SCD. Debates almost SCD tend to take identify in isolation from more mainstream debates about chronic illness. SCD has much in common with other chronic atmospheric condition (see Atkin and Ahmad, 2000). Consequently, the mainstream literature on chronic illnesses tin aid brand further sense of the educational feel of those with SCD equally they regularly have to reconstitute the relationship between their body, self and affliction (Bury et al, 2005). Insights from the broader literature on chronic illness might aid compensate for the lack of specific literature on SCD and pedagogy. SCD shares similarities with conditions such equally cystic fibrosis, diabetes, asthma and rheumatoid arthritis. Successful education provision for these conditions has the potential to have like success for those with SCD.
Finally, our business relationship is a reminder that evidence exists in a context in which it assumes a social, economic, moral and political meaning (meet Bauman, 1992). Furthermore, offering an analysis of the instruction bug facing people with SCD is one matter; doing something most information technology is some other. Ofttimes there is a gap between our agreement and our willingness to human action to ameliorate practice. A commitment to change, informed by critical insight, is essential in ensuring research informs policy (see Taylor, 1994). In practical terms, focused evaluative studies exploring specific interventions would be a welcome improver to an emerging research calendar. Exploring what innovative practice occurs in this expanse would be equally valuable.
At the same time, another tension emerges: relying on bear witness to drive interventions creates the danger of doing nothing. We would not wish to stifle innovation by calling for research before such innovation is enabled, particularly since nosotros are aware of the practice of using research as an excuse for inaction, especially in debates near meeting the education and care needs of minority indigenous populations (see Atkin, 2004). There are, nevertheless, relatively few well-designed studies on which we tin base future interventions. In the absence of robust evidence, this perhaps further emphasises the of import of reconciling our existing evidence in broader practice and theoretical debates, in order to maximise the value of what we practise know.
For example, past embedding debates near education and SCD within more general word about ethnicity, multifariousness and differences, we are able to understand the extent to which ideas such as institutional racism explain inaccessible and inappropriate provision, as well as the importance of agreement how a person's cultural and indigenous groundwork enables them to make sense of having a chronic illness. A useful instance from the USA is how the original chronic care model was expanded to include additional change concepts, i of which was cultural competence (come across Congress on Improving Chronic Care, 2002, p.iii). At the same time, however, we need to have that in some means minority ethnic populations might not be that different from the general majority population. Overall improvements in education policy and practise could have benefits for everyone. Every bit, engaging with organisational and professional person culture helps explicate the dynamic tensions in enacting policy and practice (Atkin and Chattoo, 2007). Agreement this can be as of import as understanding a person's experience of SCD. This finds resonance in current debates virtually culturally competent do in wellness and social care, which emphasise the importance of getting practitioners to challenge their ain values, develop agreement and sensitivity, and use their sensation and knowledge to advisable exercise (Papadopoulos et al, 2004), while recognising the organisational context in which they work (Dominelli, 2004). The starting bespeak for successful policy and practice guidance, therefore, becomes an assay of the nowadays difficulties, an explanation of how these difficulties are currently fabricated sense of, and a presentation of culling means of making sense of the situation. This review, past providing a critical overview of current evidence, offers a starting bespeak from which to develop more informed exercise and policy in SCD and pedagogy.
Determination
A search for literature on sickle cell and school didactics produces few directly relevant references. Clinical literature seems content to read off educational consequences from the status itself, while psychological literature frames ongoing issues as ones requiring the person with SCD to adapt. In contrast, a sociological approach tends to emphasise continuities with other chronic illnesses, with the experiences of other minority indigenous pupils, and indeed with all other peers. Farther, such approaches see attitudes and behaviours equally a office not of SCD itself, nor of maladjustment, but as socially and historically derived, and thereby amenable to effecting changes through challenges to current social arrangements.
The gateway to teaching problems that is proffered past a clinical and psychological focus is one-dimensional. The focus is on educational non-omnipresence and relative failure, on physical and performative differences that mark out such children from their peers, and on concrete symptoms that frame the young person as passive and eternally vulnerable.
A noesis review, of the blazon we have conducted here, offers other avenues to explore in researching education and young people with SCD: ones that are mindful of the context for all young pupils with chronic illnesses; of the socio-economic position of minority ethnic pupils inUKschools; of the fashion in which family unit has been historically moulded past racism; of the gendered as well as indigenous mediators of chronic illnesses; and of the normalising, testing and performative ethos of current school practices. In turn, these avenues offering more plausible ways of working towards an inclusive education for young people with SCD and other chronic illnesses. This review outlines some conditions for more successful interventions, in which the emerging evidence can appoint with and develop existing examples of innovative exercise.
Acknowledgment
This newspaper was funded by the Economic and Social Research Quango (Grant RES-000–23–1486).
CONFLICTS OF INTEREST
None.
References
- Adedoyin MA (1992) Psychosocial furnishings of sickle jail cell disease among adolescents. East African Medical Journal 69:370ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“2.
- Ahmad WIU (2000) Introduction. In: Ahmad WIU (ed) Ethnicity, Disability and Chronic Illness. Buckingham: Open Academy Press, pp. 1ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“11.
- Alao AO and Dewan MJ (2003) Psychopathology in sickle cell disease. Westward African Journal of Medicine 22:334ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“7.
- Ali N, Atkin K, Craig Thou et al (2006) Ethnicity, Disability and Piece of work: examining the inclusion of people with sensory impairments from black and minority ethnic groups into the labour marketplace. London: RNIB.
- Alvesson M and SkoÃÆ'ƒâ€šÃÆ'‚¨ldber K (2000) Reflexive Methodology: new vistas for qualitative research. London: Sage.
- Anie K (2005) Psychological complications in sickle cell disease. British Journal of Haematology 129:723ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“9.
- Anie Chiliad and Light-green J (2006) Psychological therapies for sickle jail cell disease and pain. The Cochrane Library iv:CD001916.
- Anie K and Steptoe A (2003) Pain, mood and opioid medication use in sickle jail cell disease. Hematology Journal 4:71ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“3.
- Anie K, Steptoe A, Ball Due south et al (2002) Coping and health service utilisation in a Great britain report of paediatric sickle cell pain. Archives of Disease in Childhood 86:325ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“9.
- Anionwu EN (1992) Sickle cell disorders and the school child. Health Visitor 65:120ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“two.
- Anionwu EN and Atkin 1000 (2001) The Politics of Sickle Cell and Thalassaemia. Buckingham: Open up University Press.
- Armstrong FD, Thompson RJ, Zimmerman R et al (1996) Cognitive performance and brain magnetic resonance imaging in children with sickle cell disease. Pediatrics 97:864ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“seventy.
- Atkin Grand (2004) Primary health intendance and Southward Asian populations: institutional racism, policy and do. In: Ali S and Atkin K (eds) S Asian Populations and Primary Health Care: coming together the challenges. Oxford: Radcliffe Publishing.
- Atkin 1000 and Ahmad WIU (1998) Genetic screening and haemoglobinopathies: ethics, politics and practice. Social Science and Medicine 46:445ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“8.
- Atkin G and Ahmad WIU (2000) Living with sickle prison cell disorder: how immature people negotiate their intendance and treatment. In: Ahmad WIU (ed) Ethnicity, Disability and Chronic Affliction. Buckingham: Open University Press, pp. 45ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“66.
- Atkin M and Ahmad WIU (2001) Living a ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚ËœnormalÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚â„¢ life: young people coping with thalassaemia major or sickle cell disorder. Social Scientific discipline and Medicine 53:615ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“26.
- Atkin M and Chattoo S (2007) The dilemmas of providing welfare in an ethnically diverse country: seeking reconciliation in the office of a ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚Ëœreflexive practitionerÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚â„¢. Policy and Politics 35:379ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“95.
- Atkin One thousand, Ahmad WIU and Anionwu EN (1998a) Screening and counselling for sickle prison cell disorder and thalassaemia: the experience of parents and health professionals. Social Scientific discipline and Medicine 47:1639ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“51.
- Atkin K, Ahmad WIU and Anionwu EN (1998b) Service support to families caring for a kid with a sickle cell disorder or thalassaemia: the feel of health professionals, service managers and health commissioners. Health two:307ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“27.
- Atkin K, Rodney A, Cheater F et al (2006) Providing Support for People with SCD and Thalassaemia Disorders and their Families: a review of the evidence and guidance for adept practice (Project Ref. 0300078). Systematic review submitted to the Department of Health Policy Research Plan. York: University of York.
- Barakat LP, Lash LA and Lutz MJ (2006) Psychosocial adaptation of children and adolescents with sickle jail cell disease. In: Brown RT (ed) Comprehensive Handbook of Childhood Cancer and Sickle Cell Illness: a biopsychosocial approach. New York: Oxford University Press, pp. 471ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“95.
- Barbarin OA (1994) Risk and resilience in adjustment to sickle cell disease: integrating focus groups, example reviews and quantitative methods. In: Nash KB (ed) Psychosocial Aspects of Sickle Prison cell Affliction: past, nowadays and futurity directions of research. New York: The Haworth Printing, pp. 97ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“121.
- Barbarin OA, Whitten CF and Bonds SM (1994) Estimating rates of psychosocial problems in urban and poor children with sickle prison cell anaemia. Health and SocialWork nineteen:112ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“19.
- Barbarin OA, Whitten CF, Bond S et al (1999) The social and cultural context of coping with sickle cell affliction: Three. Stress, coping tasks, family functioning, and childrenÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚â„¢s adjustment. Journal of Black Psychology 25:356ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“77.
- Barrett DH, Wisotzek IE, AbelGGet al (1988) Cess of psychosocial functioning of patients with sickle cell disease. Southern Medical Periodical 81:745ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“50.
- Barry T and Elander J (2002) Pain coping strategies among patients with haemophilia. Psychology, Health and Medicine 7:271ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“81.
- Bauman Z (1992) Intimations of Post Modernity. London: Routledge. Bediako S (2007) Racial centrality and health intendance use among African American adults with sickle cell illness. Journal of Blackness Psychology 33:422ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“38.
- Boni L, Chocolate-brown R, Davies P et al (2001) Social data processing and magnetic resonance imaging in children with sickle cell disease. Journal of Pediatric Psychology 26:309ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“19.
- Braham P, Rattansi A and Skellington R (1992) Racism and Anti-Racism: inequalities, opportunities and policies. London: Open Academy Printing and Sage.
- Broome ME, Maikler Five, Kelber S et al (2001) An intervention to increase coping and reduce health intendance utilisation for school-historic period children and adolescents with sickle cell disease. Journal of National Black Nurses Association 12:6ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“14.
- Brown R, Armstrong D and Eckman J (1993) Neurocognitive aspects of pediatric sickle jail cell disease. Journal of Learning Disabilities 26:33ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“45.
- Burlew Thou, Telfair J, Colangelo L et al (2000) Factors that influence adolescent adaptation to sickle cell disease. Journal of Paediatric Psychology 25:287ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“99.
- Bury M, Newbould J and Taylor D (2005) A Rapid Review of the Current State of Knowledge Regarding Lay Led Self- Management of Chronic Illness. London: National Institute for Health and Clinical Excellence.
- Chua-Lim C, Moore RB, McCleary G et al (1993) Deficiencies in school readiness skills of children with sickle cell anaemia: a preliminary report. Southern Medical Journal 86:397ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“402.
- Collins 1000, Kaslow N, Doepke Chiliad et al (1998) Psychosocial interventions for children and adolescents with sickle prison cell illness (SCD). Periodical of Blackness Psychology 24:432ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“54.
- Congress on Improving Chronic Care (2002) Innovations in Research and Practice. www.improvingchroniccare.org/ downloads/2002_summary_copy3.pdf (accessed 1 March 2008).
- Conyard South, Krishnamurthy Grand and Dosik H (1980) Psychosocial aspects of sickle-jail cell anaemia in adolescents. Health and Social Work five:20ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“half-dozen.
- Corker EM and French Southward (1998) Disability Soapbox. Buckingham: Open University Press.
- Darr A, Atkin Yard, Taylor S et al (2005) Chronic Illness, Ethnicity and Young People: how those with a sickle cell or thalassaemia disorder negotiate the life transitions associated with growing up: evaluating evolution activity. Evaluation report (Project No: URNRG24031). Birmingham:Midlands Sickle Jail cell and Thalassaemia Social club (formerly OSCAR Birmingham).
- Davis JK and Wasserman Eastward (1992) Behavioural aspects of asthma in children. Clinical Paediatrics November:678ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“81.
- Day D and Chismark Due east (2006) The cognitive and academic impact of sickle prison cell disease. Journal of School Nursing 22:330ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“five.
- Demaine J (1989) Race, categorization and educational achievement. British Journal of Sociology of Education 10: 195ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“214.
- Section for Educational activity and Skills (2006) Maintained Master Schools Number and Percent of Children by Ethnic Group Table 32; Maintained Secondary Schools Number and Percentage of Children by Ethnic Group Tabular array 33. world wide web.dfes.gov.uk/rsgateway/DB/SFR/s000682/SFR38 ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“2006web3.xls (accessed 1 March 2008).
- Dominelli L (2004) Social Work: theory and practice for a changing profession. Cambridge: Polity Press.
- Dooley EA and Perkins Northward (1998) LetÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚â„¢s talk about needs of African American children with sickle jail cell affliction: a recognized ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚Ëœother health impairmentÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚â„¢. In: Coming Together: Preparing for Rural Special Educational activity in the 21st Century. Proceedings of the 18th American Quango on Rural Special Pedagogy, 25ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“28 March, Charleston, SC.
- Dunlop R and Bennett K (2006) Pain direction for sickle cell illness (Cochrane Review). The Cochrane Library, Issue 4. Oxford: Update Software.
- Dyson SM (1992) Blood relations: educational implications of sickle cell anaemia and thalassaemia. In: Booth T, Swann W, Masterton M et al (eds) Curricula for Diversity in Education (Learning for All one). London: Routledge, pp. 277ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“83.
- Evans C (1998) Children with sickle cell anaemia: parental relations, parentÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“child relations and kid behaviour. Social Work 33:127ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“xxx.
- Fowler MG, White JK and Redding-Lallinger R (1986) Neuropsychological deficits among schoolhouse age children with sickle cell disease. American Periodical of Diseases of Childhood 140:297ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“313.
- Franklin I and Atkin Thou (1986) Employment of persons with sickle-cell illness and sickle cell trait. Journal of the Guild of Occupational Medicine 36:76ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“9.
- Fuggle P, Shand P, Gill LJ et al (1996) Hurting, quality of life and coping in sickle cell disease. Archives of Disease in Childhood 75:199ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“203.
- Gil KM, Wilson JJ, Orringer E et al (1996) Effects of cognitive coping skills preparation on coping strategies and experimental pain sensitivity in African American adults with sickle prison cell disease. Wellness Psychology fifteen:3ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“x.
- Gil KM, Porter L, Prepare J et al (2000) Hurting in children and adolescents with sickle prison cell disease: an analysis of daily hurting diaries. ChildrenÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚â„¢s Wellness Care 29:225ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“41.
- Hasan SP, Hashmi S and Alhassen M (2003) Low in sickle jail cell illness. Journal of the National Medical Clan 95:533ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“7. Helman CG (2007) Culture, Health and Illness (5e). New York: Oxford Academy Printing.
- Helps Due south, Peterson C, Udwin O et al (2003) Psychosocial and neurocognitive aspects of sickle prison cell illness. Child and Adolescent Mental Wellness viii:11ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“17.
- Loma SA (1994) Managing Sickle Cell Affliction in Low Income Families. Philadelphia: Temple University Printing.
- Hill SA and Zimmerman MK (1995) Valiant girls and vulnerable boys: the affect of gender and race on mothersÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚â„¢ intendance-giving for chronically ill children. Journal of Marriage and Family 57:43ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“53.
- Hilton C, Osborn M and Serjeant GR (1997) Psychiatric disorder in young adults in Jamaica. International Journal of Social Psychiatry 43:257ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“68.
- Holman CF (1997) Management of the kid with sickle prison cell disease inside the school setting. Journal of Schoolhouse Nursing 13:29ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“34.
- Hughes W and Paterson Thousand (1997) The social model of inability and the disappearing body: towards a sociology of impairment. Disability and Social club 12:325ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“twoscore.
- Hurtig AL and Park KB (1989). Aligning and coping in adolescents with sickle cell affliction. In: Whitten CF and Bertles JF (eds) Sickle Cell Disease. New York: New York Academy of Sciences, pp. 172ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“82.
- Jacob E, Miaskowski C, Savedra 1000 et al (2006) Changes in sleep, nutrient intake, and activity levels during acute painful episodes in children with sickle jail cell disease. Journal of Pediatric Nursing 21:23ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“34.
- Katz ML, Smith-Whitley K, Ruzek SB et al (2002) Knowledge of stroke take a chance, signs of stroke, and the need for stroke education amongst children with sickle cell illness and their caregivers. Ethnicity and Health 7:115ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“23.
- Male monarch AA, Tang S, Ferguson KL et al (2005) An pedagogy program to increase teacher knowledge about sickle cell disease. Journal of Schoolhouse Wellness 75:11ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“14.
- Koontz K, Brusque Advertizement, Kalinyak One thousand et al (2004) A randomized controlled pilot trial of a schoolhouse intervention for children with sickle jail cell anaemia. Journal of Paediatric Psychology 29:7ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“17.
- Lee EJ, Phoenix D, Chocolate-brown W et al (1997) A comparing study of children with sickle cell affliction and their nondiseased siblings on hopelessness, depression, and perceived competence. Periodical of Advanced Nursing 25:79ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“86.
- MacDonald K (2003) Using Systematic Reviews to Improve Social Care. London: Social Intendance Constitute for Excellence (SCIE Reports: No. 4).
- Mador JA and Smith DH (1989) The psychological accommodation of adolescences with cystic-fibrosis: the review of the literature. Journal of Adolescent Health Care 10:136ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“ 42.
- Maikler VE, Broome ME, Bailey P et al (2001) ChildrensÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚â„¢ and adolescentsÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚â„¢ use of diaries for sickle cell hurting. Journal of the Society of Pediatric Nurses 6:161ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“70.
- Maxwell One thousand, Streetly A and Bevan D (1999) Experience of hospital care and treatment seeking for hurting from sickle jail cell disease: qualitative study. BMJ 318:1585ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“90.
- Midence One thousand and Elander J (1994) Sickle Prison cell Disease: a psychological approach. Oxford: Radcliffe Publishing.
- Midence K, Davies S and Fuggle P (1992) Courage in the face of crisis: sickle cell affliction. Nursing Times 88(22):46ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“8.
- Midence Grand, Fuggle P and Davies SC (1993) Psychosocial aspects of sickle cell disease (SCD) in childhood and adolescence: a review. British Journal of Clinical Psychology 32:271ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“80.
- Midence K, McManus C, Fuggle P et al (1996) Psychological adjustment and family unit functioning in a group of British children with sickle cell illness: preliminary empirical findings and a meta-analysis. British Periodical of Clinical Psychology 35:439ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“50.
- Morgan S and Jackson J (1986) Psychological and social concomitants of sickle jail cell anemia in adolescents. Periodical of Pediatric Psychology 11:429ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“39.
- Murray N and May A (1998) Painful crises in sickle prison cell disease: patientsÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚â„¢ perspectives. BMJ 297:452ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“54. Nash KB (1989) Self-assist groups: an empowerment vehicle for sickle cell disease patients and their families. Social Work with Groups 12:81ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“97.
- Nettles AL (1994) Scholastic functioning of children with sickle cell disease. In: Nash KB (ed) Psychosocial Aspects of Sickle Cell Disease. New York: The Haworth Press, pp. 123ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“40. Nettleton South (2006) The Folklore of Health and Illness. Second Edition. Cambridge: Polity Press.
- Noll RB, Ris Dr., DaviesWHet al (1992) Social interactions betwixt children with cancer or sickle cell illness and their peers: teacher ratings. Journal of Developmental and Behavioural Pediatrics 13:187ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“93.
- Noll RB, Vannatta K, Koontz G et al (1996) Peer relationships and emotional well-being of youngsters with sickle cell disease. Kid Development 67:423ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“36.
- Oliver M (1990) The Politics of Disablement. London: MacMillan.
- Palermo TM, Witherspoon D, Valenzuela D et al (2004) Development and validation of the child activity limitations interview: a measure of hurting-related functional impairment in schoolhouse-age children and adolescents. Hurting 109:461ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“70.
- Papadopoulos I, Tilki M and Lees S (2004) Promoting cultural competence in health care through a researchbased intervention in the UK. Diversity in Health and Social Care 1:107ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“16.
- Peterson CC, Palermo TMand Swift E (2005) Assessment of psycho-educational needs in a clinical sample of children with sickle prison cell illness. ChildrenÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚â„¢s Health Care 34(2):133ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“ 48.
- Pinckney RB and Stuart GW (2004) Adjustment difficulties of adolescents with sickle cell disease. Journal of Child and Adolescent Psychiatric Nursing 17:5ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“12.
- Popay J and Roen K (2003) Using Bear witness from Diverse Research Designs. SCIE Reports: No. 3. London: Social Care Establish for Excellence.
- RichardHWandBurlew AK (1997) Bookish operation amidst children with sickle cell illness: setting minimum standards for comparison groups. Psychological Reports 81:27ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“34.
- Robinson R (1999) At that place is no shame in pain: coping and functional ability in adolescents with sickle cell disease. Journal of Blackness Psychology 25:336ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“55.
- Rodrigue JR, Streisand R, Banko C et al (1996) Social performance, peer relations, and internalizing and externalizing problems among youth with sickle cell disease. ChildrenÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚â„¢southward Wellness Care 25:37ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“56.
- Imperial, C, Headings, V, Molnar, E et al (1995) Resilience in siblings of children with sickle cell disease. Periodical of Genetic Counseling 4 (three): 199ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“217.
- Samanta A, Samanta J, Johnson Met al (2005) Rheumatoid arthritis in minority ethnic groups: patterns of affliction, clinical and sociocultural features among British South Asians. Diversity in Health and Social Care 2:99ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“118.
- Schatz J (2004) Academic attainment in children with sickle cell disease. Journal of Pediatric Psychology 29:627ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“33.
- Schatz J, Brown RT, Lambert R et al (2001) Poor schoolhouse and cognitive functioning with sickle cell illness and silent cerebral infarcts. Neurology 56:1109ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“11.
- Sellick C and Howell D (2003) Innovative, Tried and Tested: a review of good practice in fostering. London: Social Care Institute for Excellence (SCIE Knowledge Reviews: No. 4).
- Serjeant GR (2001) Historical review: the emerging understanding of sickle jail cell disease. British Journal of Haematology 112:3ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“xviii. South
- hakespeare T (1995) Back to the future? New genetics and disabled people. Disquisitional Social Policy fifteen:22ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“35.
- Shapiro BS, Dinges DF and Orne EC (1995) Home management of sickle prison cell-related pain in children and adolescents: natural history and impact on school omnipresence. Pain 61:139ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“44.
- Social Intendance Institute for Excellence (2007) What is a SCIE Knowledge Review? www.scie.org.uk/publications/ knowledgereviews/index.asp (accessed 1 March 2008).
- Swain J, Finkelstein V, French S et al (2004) Disabling Barriers: enabling environments. London: Sage.
- Swain NF, Mitchell MJ and Powers SW (2006) Hurting management of sickle prison cell disease. In: Brown RT (ed) Comprehensive Handbook of Babyhood Cancer and Sickle Jail cell Disease: a biopsychosocial approach. New York: Oxford University Press, pp. 514ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“thirty.
- Taylor C (1994) Multiculturalism: examining the politics of recognition. Princeton: Princeton University Press.
- Thomas VJ and Taylor LM (2002) The psychosocial experience of people with sickle cell disease and its impact on quality of life: qualitative findings from focus groups. British Journal of Health Psychology 7:345ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“63.
- Thomas VJ, Hambleton I and Sergeant GR (2001) Psychological distress and coping in sickle jail cell disease: comparing of British and Jamaican attitudes. Ethnicity and Wellness 6:129ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“36.
- Turner B (1996) The Body and Society, second edition. London: Sage Wilkinson R (1996) Unhealthy Societies. London: Routledge.
- Williams C (2000) Doing wellness, doing gender: teenagers, diabetes and asthma. Social Science and Medicine l:387ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“96.
- Wilson RE, Krishnamurti 50 and Kamat D (2003) Direction of sickle cell illness in primary care. Clinical Pediatrics 42:753ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“61.
- Wjst K, Roell G, Dold S et al (1996) Psychosocial characteristics of asthma. Journal of Clinical Epidemiology 49:461ÃÆ'ƒÂ¢ÃÆ'‚€ÃÆ'‚“6.
Source: https://www.primescholars.com/articles/education-and-young-people-with-sickle-cell-disorder-a-knowledge-review-94696.html
0 Response to "English I – Unit 10 Review Library Skills and Visual Aids"
Post a Comment